
Returning to work…life…play
Return to Work Clinical Practice Guidelines: Published October 2021 (Hot off the press!)
Data from 2018 from the US Bureau of Labor Statistics (BLS)identified more than 2.8 million nonfatal workplace injuries and illnesses, with more than 900 000 occupational injuries and illnesses requiring time away from work and another 700000 cases involving job transfer or restriction. Occupations with the highest number of injuries include laborers, heavy and light truck drivers, nursing assistants/nurses, order fillers/stockers, retail sales, maintenance, construction, and cleaners. The distribution of injuries and illnesses in 2018, categorized by body part, showed that injuries of the upper extremity were most common at 32%, followed by lower extremities (24%), trunk (22%), multiple body parts (10%), head and neck (10%), and body systems (2%). Falls, slips, and trips accounted for 27% of the private occupational injuries and illnesses in 2018.
Active claims data from the National Safety Council showed that 2.5 million incidents of work-related injuries during 2018 resulted in 105 million lost workdays!
At the clinic we believe in full transparency related to injury recovery. Here is the best, most up to date comprehensive information to help us and you!
Yikes…..So how can we help you?
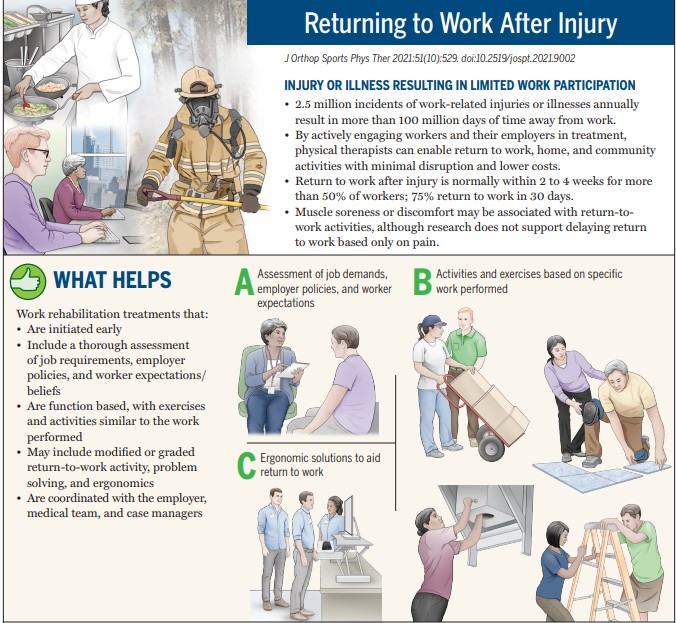
• By actively engaging workers and their employers in treatment, physical therapists can enable return to work, home, and community
activities with minimal disruption and lower costs.
• Return to work after injury is normally within 2 to 4 weeks for more than 50% of workers; 75% return to work in 30 days.
• Muscle soreness or discomfort may be associated with return-to-work activities, although research does not support delaying return to work based only on pain.
Return to work key points for patients:
Return to work Clinical Perspectives: The bottom line for us to help you the most.
Job demands and functional assessment should be used to develop a work-limiting diagnosis and treatment goals. In addition to risk factor screening, valid and reliable self-report measures should specifically address RTW. Graded, modified, or transitional duties that promote work reintegration should be included in the plan of care. A combination of condition-specific exercise and work-focused interventions (work task replication) is indicated for workers with an estimated low risk of delayed RTW. A behavioral approach with a combination of clinic-based, work-
focused interventions and jobsite interventions is indicated for those considered at high risk for delayed RTW. Psychologically informed practice should include individual goal setting, motivational interviewing, activity pacing, problem solving, relaxation, and coping techniques.

